Suzie's medical and family history
Previous medical history
- 2 children aged 10 and 13 - SVD with no complications
- Migraine headaches - infrequent, with aura
- Single episode of iritis in the past
- Polycystic ovary seen on ultrasound 15 years ago
Medications
- Aspirin 900mg at the onset of a migraine taken with Maxolon 10mg
- No regular medications
Social History
- Married: husband Paul has had a vasectomy
- Smoker (5/day)
- Has her own accounting practice
Family History
- Sister has coeliac disease
- Mother has recurrent iritis and hypothyroidism
Exploring Suzie's symptoms further
I would ask Suzie about:
- More about her fatigue symptoms
- Mood: Is there any depression or anxiety?
- Weight: any changes?
- Appetite: any changes?
- Cold intolerance
- Hair loss
- Joint pains
- Past history of postpartum thyroiditis
- Hot flushes
- Further history around her menstrual cycle symptoms
- Palpitations
- Headache
Physical examinations
Examinations should include:
- Blood pressure
- Pulse
- Weight
- Palpation of the thyroid gland
- Conjunctival pallor
To exclude other causes you might also like to perform:
- Joints examination
- Mental health assessment
- Temperature measurement
- Abdominal exam
- Pelvic examination
Signs and symptoms of hypothyroidism 1
| System | Signs and symptoms |
|---|---|
| Appearance |
|
| Energy/metabolism |
|
| Nervous system |
|
| Cognitive/Psychiatric |
|
| Cardiovascular |
|
| Musculoskeletal |
|
| Gastrointestinal |
|
| Reproductive system |
|
| Investigation results (other than TFTs) |
|

Causes of hypothyroidism
Worldwide, iodine deficiency is the most common cause of hypothyroidism.
In Australia autoimmune chronic lymphocytic thyroiditis is the most common aetiology of hypothyroidism.
Increased risk of thyroid disease includes those with:
- A history of autoimmune disease
- Past history of head and neck irradiation
- Previous radioactive iodine therapy
- Presence of a goitre
- Family history of thyroid disease
- Treatment with drugs known to influence thyroid function e.g. amiodarone, lithium
So, M., MacIsaac, R.J. and Grossmann, M. (2012). Hypothyroidism: Investigation and management. Australian Family Physician, 41(8), 556-562.
Which investigations you should consider
To rule out or confirm thyroid dysfunction:
- Thyroid stimulating hormone (TSH) blood test
Initial screening is done by measuring the patient's TSH level. If this is elevated, identify which further tests are required.
To exclude other concerns:
- FBC and Fe studies
- ELFT: Renal or liver dysfunction
- ESR or CRP: Inflammatory joint disease
- Glucose: Diabetes
- Antinuclear antibodies (ANA): May be appropriate given Suzie's past history of menorrhagia (refer to the online module on 'Menstruation and Abnormal PV Bleeding')
There is no evidence that screening asymptomatic adults improves outcomes.
Investigations that may be inappropriate or premature
Inappropriate investigations:
- Free T4
- Free T3
- TSH receptor antibodies
- Thyroid peroxidase antibody
- Any thyroid imaging
Any other testing at this stage is premature e.g.:
- B12
- ENAse DNAse
- CCP
- Rh factor
- Serology for viral illnesses
Working diagnosis for Suzie
Suzie's TSH level of 6.0 mIU/L is elevated (i.e. > 4.0 mIU/L).
My working diagnosis is subclinical thyroiditis.
As Suzie is symptomatic, further investigation is required to confirm the diagnosis.
The next thing I would do is to:
- Obtain a free T4 level immediately
- Consider checking TPO antibody
- Consider offering 3-6 month trial of levothyroxine and continue if symptomatic benefit
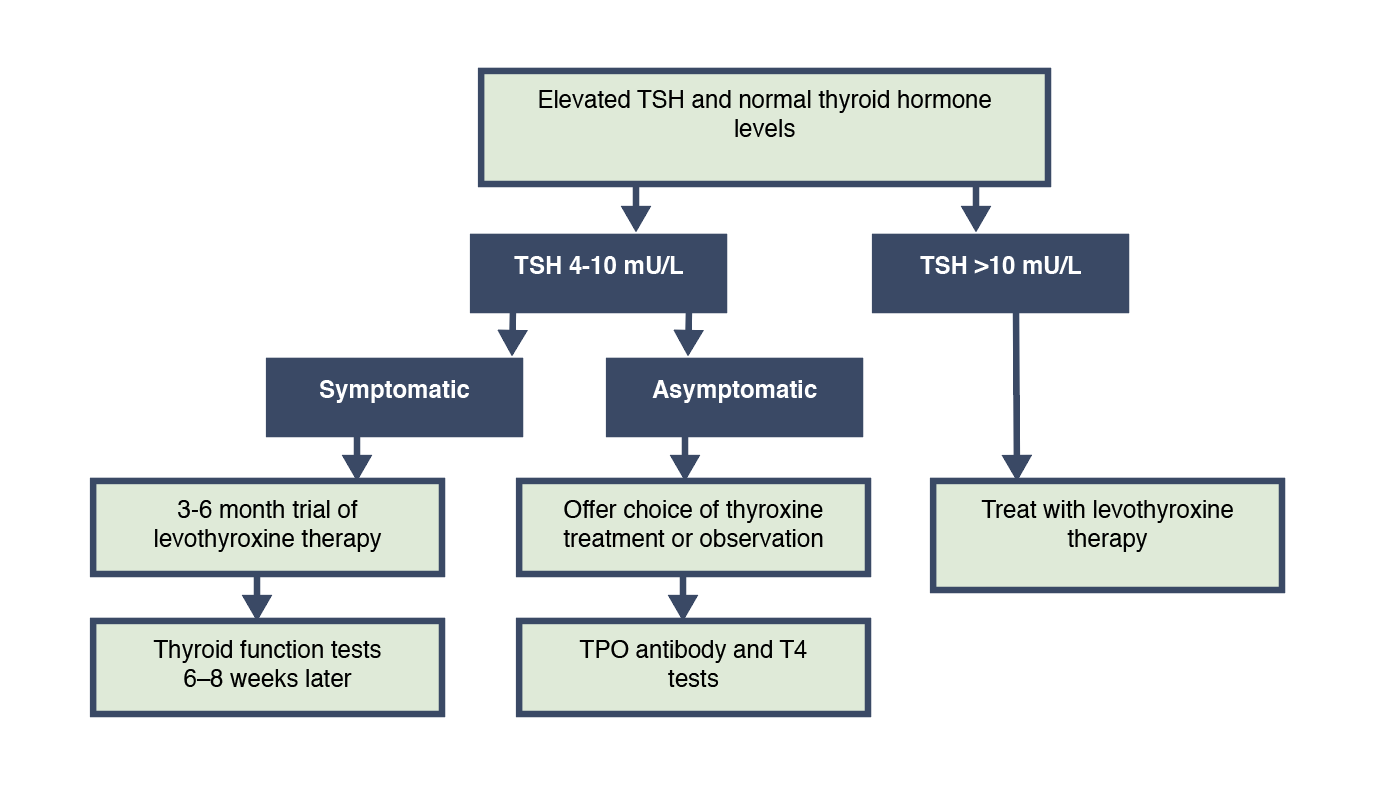
Treating patients with mildly elevated TSH (4-10 mU/L):
- The significance and hence the benefits of treating subclinical hypothyroidism remains controversial1
- If TSH is 4-10 mU/L in an asymptomatic individual, manage as follows;
- Check serum TSH, free T4 and TPOAb 6-8 weeks later.
- Offer treatment if the abnormality persists.
- The health impact of subclinical hypothyroidism with mildly elevated levels of TSH (4–10 mU/L) remains uncertain, particularly in older people; treatment or observation are reasonable options2.
- In patients with a mildly elevated TSH (up to 10 mU/L), TSH normalises without treatment in over 50% of cases, so treatment need not be offered immediately.


Interpreting hypothyroid function test results

Figure 1. Interpretation of hypothyroid function test results
Management of subclinical hypothyroidism
Thyroid HRT (hormone replacement therapy)
Most patients with hypothyroidism will require lifelong thyroid hormone replacement therapy
- Measurement of both TSH and free T4 is required to optimise therapy
- The normal thyroid gland makes two hormones:
- T3: the biologically active form
- T4: produced in greater amounts
- Approximately 80% of T3 is derived by the peripheral conversion of T4. Synthetic T4 also undergoes deiodination in the periphery to the biologically active T3
- The normal thyroid gland makes two hormones:
- Replacement therapy with thyroxine (Levothyroxine or LT4) is the basis of therapy
- Thyroxine should be administered at a dose of 1.6μg/kg lean body weight daily, taken on an empty stomach
Repeat TSH testing
The optimal dose of thyroxine for long-term therapy is assessed from results of thyroid function tests together with clinical findings. The optimal dose of thyroxine should result in a TSH in the detectable range, not elevated and preferably within the reference range.
- Repeat TSH testing in 6-8 weeks
- The minimum period to achieve a stable concentration with thyroxine is 2 months
- If TSH is in the normal range
- Dose is appropriate and annual serum TSH should be carried out to monitor the patient
- If TSH is >5.0 mIU/L, patient is under-replaced
- Check compliance and if patient is adherent, increase dose by 12.5 - 50mcg daily or second daily. Recheck in 6-8 weeks
- If TSH <0.35 mIU/L, patient is over-replaced
- Decrease daily dose by 12.5 - 50mcg daily or second daily and recheck in 6-8 weeks
- Once a patient is stabilised on therapy, TSH readings should be taken at least annually
When a referral to an endocrinologist is indicated
Patient is aged less than 18 years
Patient is unresponsive to therapy
Pregnancy
Presence of other endocrine disease
Presence of goitre, nodule or other structural changes to the thyroid gland
Thyroid disease in the perinatal period
- Pregnancy is a state of increased thyroid demand (thyroid hormone synthesis is increased by up to 50%)
- Iodine requirements are increased in pregnancy (WHO recommends a daily intake of 250mcg during pregnancy and lactation). Excess iodine can cause fetal hypothyroidism so very large doses (Kelp tablets, Lugol's iodine solution) should be avoided
- Pregnancy specific reference ranges should be used
- Untreated hypothyroidism results in children with a decreased IQ and increases the risk of miscarriage, premature birth, stillbirth, and low birth weight
- Women with pre-existing hypothyroidism need to increase their thyroxine dose by 30% in pregnancy – this equates to 2 additional doses per week on suspicion or confirmation of pregnancy
- TSH and free T4 should be rechecked every 4 weeks for the first half of pregnancy and then again at 26-32 weeks
- After delivery, the thyroxine dose can be reduced to pre-pregnancy levels. If adequately treated through pregnancy, neonatal thyroid function testing is not necessary
- Subclinical hypothyroidism is associated with miscarriage, but not impaired cognitive function. Some clinicians may choose to consider low dose thyroxine replacement but clear guidelines have not been established
- Overt hyperthyoidism in pregnancy is less common and may be due to Graves' disease, a toxic nodule or gestational thyrotoxicosis
- Postpartum thyroiditis is common, affecting 1 in 20 women. Presentation may be hypothyroid (48%), biphasic (hyperthyroidism followed by hypothyroidism) (22%) or isolated hyperthyroidism (30%)
- Postpartum thyroiditis with hyperthyroidism usually occurs 3-6 months postpartum and needs to be differentiated from Graves' disease. Beta blockers can be used for symptomatic management and the thyrotoxic phase tends to self-limit.
- Postpartum thyroiditis resulting in hypothyroidism usually occurs at 6-12 months postpartum. Thyroxine is indicated for those trying to conceive or those experiencing symptoms. A high proportion of women will recover. An attempt to wean thyroxine 6-12 months after the final pregnancy should be made. Long-term follow up with annual TFT is recommended


Hypothyroidism
Occurs in about 5% of the adult population; women to men 5:1 (i.e. up to 8% women and 2% of men)
Initial screening is performed by measuring TSH
Subclinical hypothyroidism (mild thyroid failure) is the most common. Raised TSH but normal T4
Overt hypothyroidism: Raised TSH and decreased T4
Secondary hypothyroidism: Normal TSH and low T4. Suggests a pituitary or hypothalamic cause or a severe non-thyroidal illness
Autoimmune chronic lymphocytic thyroiditis is the most common cause in Australia (characterised by raised circulating levels of thyroid peroxidase antibody)
Symptoms and signs are often mild or subtle
Thyroid function tests are needed to confirm the diagnosis
If serum TSH level is raised, free T4 and thyroid peroxidase antibody should be measured (this is the only test needed to confirm the diagnosis of autoimmune thyroiditis)
A diagnosis of hypothyroidism in itself is not an indication for thyroid imaging. Thyroid ultrasound is only indicated to evaluate structural thyroid abnormalities (e.g. palpable thyroid nodules)
Replacement therapy with thyroxine is the basis of therapy (1.6μg/kg lean body weight daily, taken on an empty stomach)
Measurement of both TSH and free T4 is required to optimise therapy
The minimum period to achieve a stable concentration with thyroxine is 2 months, (thyroid function tests should not normally be requested before this period elapses)
Optimal dose for long-term therapy: assessed through thyroid function tests and clinical findings.
Optimal dose of thyroxine should result in a non-elevated TSH level in the detectable range (preferably within the reference range)
Once a patient is stabilised on therapy, TSH readings should be taken at least annually
Free T3 testing is not necessary in the assessment of hypothyroidism or during routine thyroxine replacement
Signs and symptoms of thyrotoxicosis
- General - Weight loss, sweaty skin, heat intolerance
- Psychiatric - Anxiety/ irritability
- Musculoskeletal - Muscle weakness, proximal myopathy
- Skin - Vitiligo, thin skin, pretibial myxoedema
- Cardiovascular - Tachycardia, AF, heart failure, systolic hypertension
- Endocrine - Goitre, gynaecomastia
- Gynaecological - Oligomenorrhoea
- Neurological - Tremor
Evaluation of thyrotoxicosis
- TSH (decreased)
- Free T4 (elevated)
- TSH receptor antibody (90-99% sensitivity in Grave’s Disease)
- Radionuclide thyroid scan
Refer to the flow chart on the evaluation of thyrotoxicosis.
{kind=link}
Differential diagnoses for thyrotoxicosis
- Sepsis, possibly urosepsis
- Heat stroke
- Thyroid storm
Treating thyroid storm
Treatment involves:
- block hormone synthesis and release
- decreasing conversion of thyroxine (T4) to triiodothyronine (T3)
- controlling tachycardia and rate-dependent heart failure
- restoring hydration
- giving sedation if needed
General supportive measures include:
- aggressive fluid rehydration, correct electrolyte imbalances
- benzodiazapines if agitated
Thyroid specific – The 5 B’s
- Block Synthesis
- PTU 600-1000mg loading dose, then 200mg orally 4 to 6 hourly
- Block Release
- Lugol solution 0.5mL orally, 3 times daily
- Block Conversion
- Dexamethasone 4mg orally or IV, 12 hourly
- Beta-blockers
- Propranolol 40 – 80mg orally, 4 times daily
- Block Enterohepatic Circulation
- Cholestyramine 4g orally, 6 hourly