Patient history
Penny is a 45-year-old woman
She has had asthma since she was a small child
She uses salbutamol 2-4 puffs most days to relieve wheezing and tightness in the chest
Penny's full medication profile
Fluticasone 250mcgs MDI 2 puffs BD
Salbutamol 100mcgs MDI prn
Ibuprofen prn for some intermittent knee pain
Background information on asthma
Asthma is a common chronic inflammatory lung disease, which can be controlled but not cured. Asthma is defined by the presence of both the following:
- Excessive variation in lung function (variable airflow limitation e.g. variation in expiratory airflow that is greater than that seen in people without asthma)
- Respiratory symptoms (e.g. wheeze, shortness of breath, cough, chest tightness) that vary over time and may be present or absent at any point in time
The underlying pathophysiology involves airway hyper-responsiveness and intermittent airway narrowing due to bronchoconstriction, small airway oedema, mucus hypersecretion, smooth muscle hypertrophy and epithelial desquamation.
The prevalence of asthma in Australia is relatively high, by international standards. 11% of the Australian population has asthma — about 1 in 10 adults and about 1 in 9 or 10 children.
Asthma is more common in Aboriginal and Torres Strait Islander peoples. 16% of Aboriginal and Torres Strait Islander people have asthma. The prevalence is 1.6 times that in non-indigenous Australians.
Asthma tends to be more prevalent in people living in lower socioeconomic areas.
There is a strong link between asthma and allergy and asthma and allergic rhinitis.
Asthma is more common in people with a family history of asthma.
Despite the known additional health risks, just as many non-smokers have asthma as smokers.
It is sometimes be difficult to distinguish between asthma and chronic obstructive pulmonary disease (COPD).


Diagnosis of asthma
There is no 'gold standard' for the diagnosis of asthma. The diagnosis of asthma is based on history, physical examination, considering other diagnoses and documenting variable airflow limitation.
Spirometry is the lung function test of choice for diagnosing asthma and for assessing asthma control in response to treatment.Young children cannot perform spirometry. Spirometry can usually be performed from age 6 years and older.
A diagnosis of asthma can be made in an adult when:
- The person has variable symptoms (especially episodes of cough, chest tightness, wheeze and shortness of breath)
- Variable airflow limitation is demonstrated on spirometry
- There are no findings that suggest an alternative diagnosis.
It can sometimes be difficult to differentiate between asthma and COPD and there can sometimes be overlap in older adults.
A normal physical examination does not exclude asthma.
Performing spirometry
Spirometry should be performed by trained staff using calibrated equipment.
Before an appointment for spirometry is booked:
- Patient should be advised to bring their own spacer and reliever
- Without bronchodilators as per Spirometry Quick Reference Guide - a guide to performing high quality spirometry National Asthma Council
The staff member should:
- Check spirometer is set up correctly and perform calibration
- Attach disposable filter and mouth piece
- Enter patient information:
- Height
- Weight
- Date of birth
- Sex at birth
- Ethnicity
- Smoking status
- Record time patient last used bronchodilator
- Give clear instructions and demonstrate correct postures and process
- Explain to patient that they will need to repeat the process at least 3 times to get a reliable result (maximum 8).
- Offer a nose clip for patient to use (recommended but not essential)
For open circuit method, which measures expiration only, the patient should:
- Sit upright with feet firmly on the floor and not lean forward
- Breathe normally for 2-3 breaths
- Breathe in rapidly and deeply to completely fill their lungs
- Put the mouthpiece in their mouth and close their lips, forming a good seal Without pausing for more than 2 seconds, blast air out as hard and fast as possible and for as long as possible, until the lungs are completely empty. They need to keep blowing until they cannot blow any more.
- Remove mouth piece
- Breathe normally and relax
Acceptable blows must be smooth continuous expiration of maximal lung volume:
- Expiration been performed with a good start, without coughing
- Forced expiration has been maintained throughout the test
Repeat the test until you obtain three reproducible and acceptable measures, where:
- The 2 largest values for FVC should be within 150 mL of each other
- The 2 largest values of FEV1 should be within 150 mL of each other.
Testing is complete when acceptability and reproducibility criteria are met. 8 is the maximum number of trials in adults.
Recording the results
Record the best forced expiratory volume in one second (FEV1) and FVC obtained.
Assessing for reversibility
- Perform baseline spirometry as per above instructions
- Administer bronchodilator- use patient's own inhaler and spacer
- give four separate doses of salbutamol 100 mg via a metered-dose inhaler (MDI) and large-volume spacer. (A large-volume spacer is more efficient.)
- Wait 10-15 minutes
- Repeat spirometry
- Repeat the test until you obtain three reproducible and acceptable measures, where:
- The 2 largest values for FVC should be within 150 mL of each other
- The 2 largest values of FEV1 should be within 150 mL of each other.
- Testing is complete when acceptability and reproducibility criteria are met. 8 is the maximum number of trials in adults.
- Repeat the test until you obtain three reproducible and acceptable measures, where:
Recording the results post-bronchodilator and calculate reversibility
Record the best forced expiratory volume in one second (FEV1) and FVC obtained post-bronchodilator.
Calculate percentage and absolute increase in FEV1

Airflow limitation is judged to be reversible if either of the following applies:
- Baseline FEV1 >1.7 L and post-bronchodilator FEV1 at least 12% higher than baseline
- Baseline FEV1 ≥1.7 L and post-bronchodilator FEV1 at least 200 mL higher than baseline
Results should be expressed as absolute values and also as a percentage of predicted values, based on the patient's age, height and sex.

Medicare billing:
To claim a 11505 to diagnose asthma, spirometry must be recorded both pre and post bronchodilator. This can only be claimed once in a 12-month period.

Trigger factors
Common triggers include:
- dust / dust mite
- cigarette smoke
- pollen
- animal dander
- feathers
- moulds
- certain foods
- respiratory viral infections
- medication such as NSAIDS
Consider occupational asthma in any cases of adult-onset asthma or in the following occupations: animal handlers, nurses, bakers and pastry makers, spray painters, chemical workers, timber workers, food processing workers and welders — is there a possible trigger at work (i.e. do the symptoms improve on days off)?
Delivery devices
Asthma medication is usually administered by inhalation:
- Metered-dose inhaler (MDI) with or without the use of a spacer
- Dry-powder inhaler (DPI)
Provided the devices are used correctly, there is no evidence of long-term clinical advantage of one device over another. (*1)
In general, patients with adequate inspiratory force and adequate hand-lung coordination can use either a DPI or an MDI.
For older patients who have inadequate inspiratory force and/or poor coordination, use of an MDI with a spacer is preferred. Alternatively, a breath-activated MDI may warrant consideration.
For patients who have arthritis in their hands or have difficulty holding the inhaler, a device like the Haleraid (pictured left) or Turboaid might be useful.

Checking inhaler technique
In an Australian study, 75% patients using an inhaler for an average of 2–3 years reported they were using their inhaler correctly but, on objective checking, only 10% demonstrated correct technique. (*1)
To help patients use their inhaler correctly:
- Ensure your own knowledge of inhaler technique is up-to-date
- Ensure inhaler is appropriate for the patient
- Ask the patient to bring in their devices and observe their technique
- Give patients verbal instructions (not just a leaflet)
- Give a physical demonstration (placebo devices are often available in practices or, if not, from pharmacies and drug representatives)
Be aware of common errors for each type of inhaler
e.g. Keep chin up and inhaler upright (not aimed at roof of mouth or tongue)

Common errors
Common errors with MDI include:
- Inability to coordinate activation with inhalation
- Failure to hold breath for a sufficient time
- Multiple actuations without waiting or shaking in between doses
- Incorrect position of inhaler
- Failure to close lips to form a good seal
- Difficult for people with osteoarthritis affecting hands
- May be unsuitable for patients with a poor inspiratory flow rate (e.g. COPD)
Confirming the diagnosis
Before starting preventer treatment, confirm the diagnosis of asthma if possible (unless symptoms are severe).
For patients who report the diagnosis of asthma made in the past or elsewhere, confirm the diagnosis if possible.
For a patient with a diagnosis of asthma and new respiratory symptoms, confirm the symptoms are due to asthma.
For a patient with a diagnosis of asthma, check symptom control.
Discussing complementary therapies with patients
- Ask about use of complementary medicines and advise patients about potential hazards.
- Encourage a good therapeutic partnership with the patient by asking the patient use of complementary therapies in an open, non-judgemental approach.
- There is insufficient evidence to support complementary therapies as asthma treatments and in some cases insufficient safety data.
- Some complementary medicine such as royal jelly may cause severe reactions and should be used with caution in asthmatics.
Penny's treatment
Penny is already on high-dose inhaled corticosteroid (ICS) medication. ICS medications have a flat dose-response curve; increasing the dose at the top end of the curve produces relatively small improvements in lung function.
Consider adding a long-acting beta2agonist (LABA) to a medium-dose ICS before using a high-dose ICS for uncontrolled asthma. The dose for Penny would be salmeterol 50 micrograms twice a day, or eformoterol 12 micrograms twice a day.
As Penny has not achieved control with a high dose ICS, it would be important to assess other factors that may be contributing:
- We have discussed checking technique and triggers.
- Has there been a recent viral exacerbation? If so, consider a course of oral steroids.
- Are her symptoms really due to asthma or could they be due to GORD or anxiety?
Stepped approach to treatment
Before considering stepping up, check:
- Symptoms are due to asthma
- Inhaler technique is correct
- Adherence is adequate
- Trigger avoidance is being attempted
Consider stepping up if good control is not achieved.
When asthma is stable and well controlled for 2-3 months, consider stepping down (e.g. reducing inhaled corticosteroid dose, or stopping long-acting beta2agonist if inhaled corticosteroid dose is already low).
Penny's diagnosis
Diagnosis
- Acute severe asthma
Differential diagnoses
- Left ventricular failure
- Anaphylaxis
- Aspiration
- Inhaled foreign body (unlikely)
- Pulmonary embolism
- Panic attack, anxiety or hyperventilation syndrome
- Pneumothorax
Initial management of acute severe asthma
- DRSABC approach
- Commence oxygen immediately and start salbutamol nebulizers (continuous). Titrate to >92%
- Obtain IV Access – point of care testing (blood gas, monitor K+) and formal blood tests (ie FBC, E/LFTs) if indicated (specifically looking for Mg2+)
- CXR – as severe asthma is indicated
- Consider salbutamol infusion (bolus 250mcg then 1-20mcg/min)
- Nebulised Atrovent 500mcg q2-6 hourly
- If not improving after Ipratropium Bromide – for Magnesium IV infusion – 10mmol over 20 minutes
- Steroid load – 50mg prednisolone if can tolerate oral (daily) – if not, for 200mg IV hydrocortisone (q6h)
- Aminophylline – 6mg/kg load → 0.5mg/kg/hr (check levels daily, aim 30-80micromol/L)
Other suggestions
- Adrenaline – nebulised 5mg, SC 0.5mg, IV – load with 1mg → 1-20mcg/min
- Ketamine – 0.5-2mg/kg/hr
- Inhalational agents – sevoflurane, anaesthetic machine or custom fitted ventilator required
Intubation
- Call for help (ideally an on-call anaesthetist)
- Use IV ketamine for induction agent if possible (can help with bronchodilation). Propofol is an alternative (but can cause hypotension)
- Try and use non-invasive ventilation for pre-oxygenation (delayed sequence induction). Can try high flow nasal prongs if available for pre-oxygenation
- Use large endotracheal tube when intubating if possible
- Monitor lung pressures when intubated closely
- Sedation while intubated and paralyzed
Initial ventilator settings:
- RR 10
- Short inspiratory time (flow rate 80-100L/min) → high peak airway pressure but low plateau pressure → decreased barotrauma
- I:E (Inspiratory:Expiratory) of 1:>4
Gas trapping
- Gas-trapping occurs because the low expiratory flow rates mandate long expiratory times if the entire inspired volume is to be exhaled. If the next breath interrupts exhalation, then gas-trapping results1:
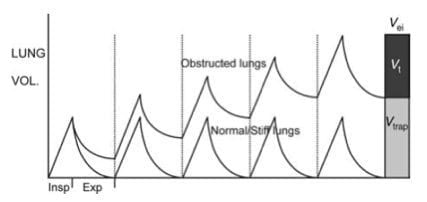
- Because gas is trapped in the lungs there is additional pressure at the end of expiration (auto-PEEP or intrinsic PEEP) above applied PEEP, which leads to dynamic hyperinflation.
- Dynamic hyperinflation has been defined as failure of the lung to return to its relaxed volume or functional residual capacity at end-exhalation.2

